
by JoAnn Gurenlian, RDH, MS, PhD, AAFAAOM, FADHA
May 29, 2024
Members of the American Academy of Pediatrics, Section on Oral Health, Council on Child Abuse and Neglect, provided a clinical report to review the oral aspects of abuse and neglect in children and the role of pediatricians, dental professionals, and other physicians in recognizing and evaluating such conditions. This clinical report noted that child abuse and neglect affect at least one out of seven children in the United States (US).1 Children may be exposed to multiple kinds of maltreatment that manifest in the mouth including physical and sexual abuse, dental neglect, medical child abuse, bullying and human trafficking.
It is important for all health care providers, including oral health professionals, to be alert to and knowledgeable about signs and symptoms of child abuse and neglect, and to know how to respond to these conditions. In the US, these health care professionals have a legal requirement to report suspected child abuse and neglect to child protection authorities. Recognizing physical abuse in children can be challenging. The majority of injuries involve bruising to the face, forehead, or ear.
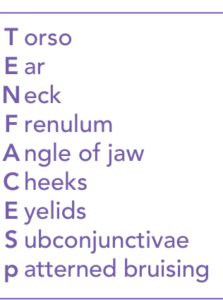
Mneumonic for identifying abuse.
The mnemonic TEN-4-FACESp can be used to identify abuse. This mnemonic stands for Torso, Ear, Neck, Frenulum, Angle of jaw, Cheeks, Eyelids, Subconjunctivae in children younger than 4 years, bruising anywhere in infants younger than 5 months, or patterned bruising. Orofacial injuries that signal abuse may include occult fractures, central nervous system injuries, contusions, burns or lacerations of the tongue, lips, buccal mucosa, palate, gingiva, alveolar mucosa or frenum, fractured, displaced or avulsed teeth, or facial bone and jaw fractures. Evidence of sexual abuse is represented by the acquisition of sexually transmitted infections and testing should be performed.
Medical Child Abuse (MCA) or Munchausen syndrome by proxy, and caregiver fabricated-illness is also a form of child mistreatment. Oral manifestations of MCA can include recurrent mucosal bleeding and ulcerations, mucosal desquamation, drooling and dysphagia due to the administration of forced ingestion of poisons. Bite marks on the skin that are acute or healed may indicate abuse. Children with orofacial or dental abnormalities are frequently subjected to bullying which may result in serious psychological effects including depression and suicide ideation. Human trafficking is another major global health issue with dental ramifications. Survivors may experience a higher risk of STIs, unsafe abortions, malnutrition, untreated medical disorders, and tooth loss, poorly formed teeth, dental caries and infections.
Dental neglect is the most frequent type of abuse seen by dental professionals and can be challenging to identify. The point at which to consider a person negligent and begin intervention is after the parent has been properly alerted by a pediatrician, dental professional, or other physician about the child’s condition, the specific treatment needed, and the means to access that treatment.
The authors proposed nine recommendations in the clinical report. Examples of these include:
- Pediatricians, dental professionals, and other physicians must report injuries that are concerning for abuse or neglect to child protective services in accordance with local or states legal requirements.
- Children with dental abnormalities are at increased risk for bullying. Therefore, providers should ask their patients about bullying and advocate for antibullying prevention programs in schools and other community settings.
- Children who have experienced human trafficking may visit a variety of health care settings. Health care providers and dental professionals are encouraged to be aware of human trafficking screening tools and the risk factors for human trafficking to identify children at risk and to safely report and connect patients to resources.
- If parents do not obtain necessary treatment for a child’s oral or dental disease after barriers to care have been addressed, the case should be reported to the appropriate child protective services agency as concerning for dental neglect.
To learn more about child abuse and neglect, read the clinical report here.
____________________________________
Reference:
1Centers for Disease Control and Prevention. Fast Facts: Child abuse and neglect prevention. Available at: https://www.cdc.gov/child-abuse-neglect/about/index.html. Accessed May 28, 2024.
____________________________________
This article summarizes the research article “Oral and Dental Aspects of Child Abuse and Neglect,” as published online in Pediatrics, Volume 140, Issue 2, August 01, 2017. (https://doi.org/10.1542/peds.2017-1487)
JoAnn Gurenlian, RDH, MS, PhD, AAFAAOM, FADHA, is the ADHA Director of Education, Research and Advocacy, professor emerita in the Department of Dental Hygiene at Idaho State University, and past president of the American Dental Hygienists’ Association, 1990-1991.


